How AI Is Actively Changing What Physicians Prescribe In 2026
AI is changing what physicians actually prescribe. Here's what the research shows and what Canadian pharma teams need to do about it.
By the team at PharmaServ
A physician walks into a patient visit with a treatment already in mind. They open the EHR to write the script, and the system surfaces a different recommendation. In a large share of cases, what gets prescribed changes.
That moment is baked into clinical workflows at hospitals and outpatient practices across Canada, and it has consequences that pharma teams have been slow to fully absorb.
From Background Tool to Treatment Influence
Clinical AI started as reference support: drug interaction checkers, guideline summaries, differential diagnosis aids. That role has expanded. AI tools now sit inside the prescribing workflow itself, ranking medication options before a physician has finished weighing alternatives, flagging safety concerns that redirect choices, and summarizing guideline pathways in ways that narrow what a clinician even considers.
Helping a physician look something up is one thing. Shaping the shortlist of what they prescribe is another.
The Research That Changes the Conversation
A study published in NPJ Mental Health Research found that 66.7% of physicians changed their treatment decision when an AI tool disagreed with their initial assessment. Two in three physicians reconsidering a plan they had already formed, not because new patient information came in, but because an algorithm pushed back.
That number reframes the HCP engagement challenge for any pharma team. It is no longer enough to make sure physicians know a therapy exists. The relevant question is whether the AI tools they rely on will surface it, rank it appropriately, or flag a concern that drops it down the list.

Why Physicians Follow AI More Often Than You Would Expect
The 66.7% figure is striking, but it reflects conditions familiar to anyone who has spent time in a clinical setting.
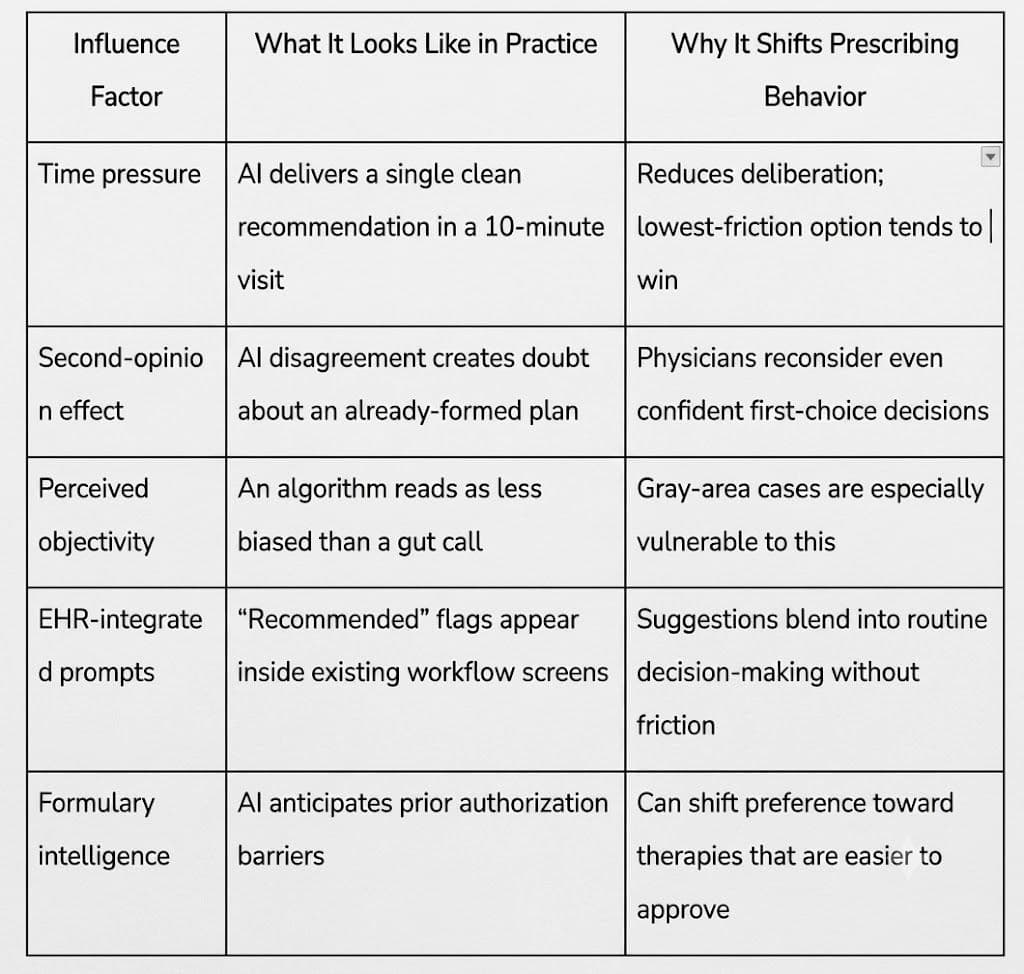
No single factor is decisive on its own. Together, they create a clinical environment where following the AI recommendation is the path of least resistance, particularly under time pressure or diagnostic uncertainty.
How AI Narrows the Prescription Landscape
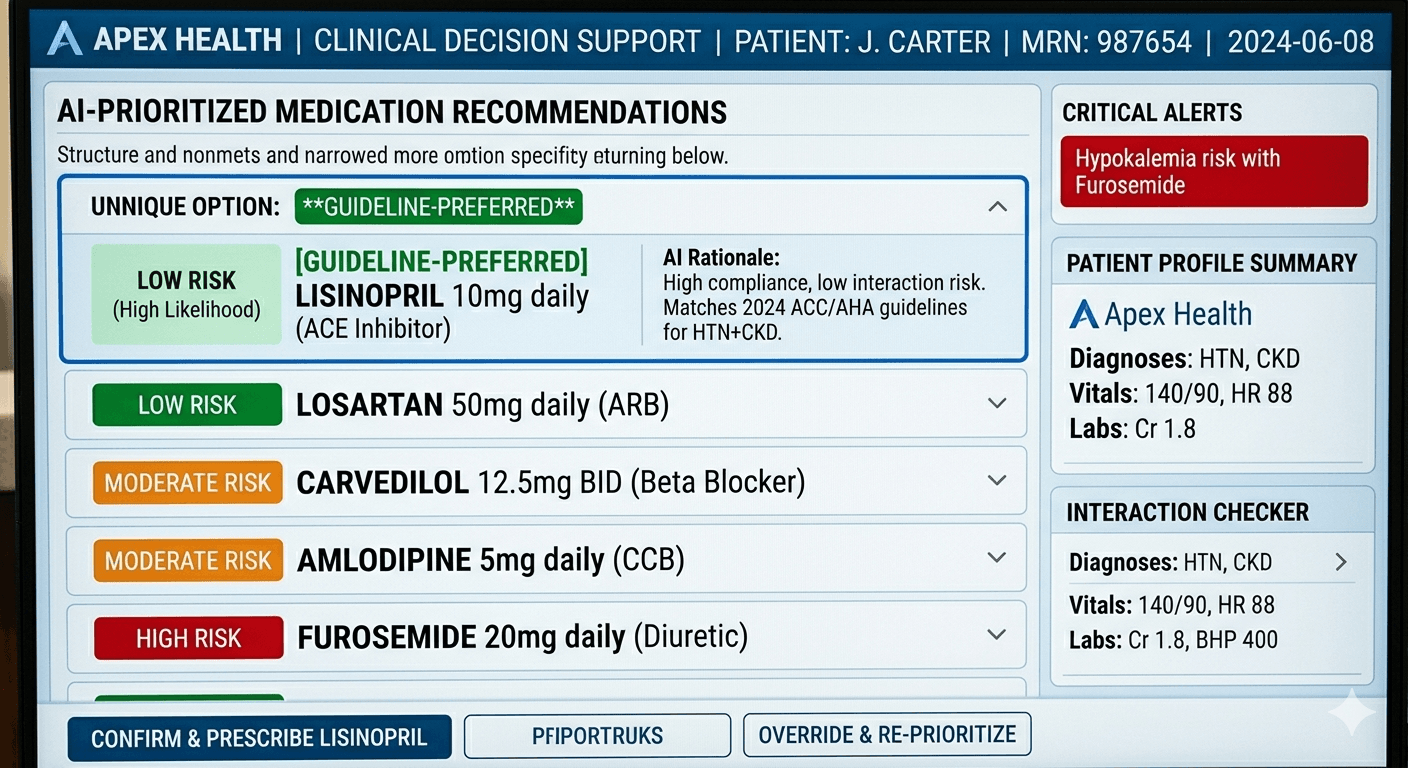
The influence is not just a pop-up a physician can dismiss. Medication ranking pushes certain options to the top before alternatives are fully considered. Risk flags redirect prescribing away from therapies that might otherwise suit a specific patient. Guideline pathway tools collapse the decision space to on-pathway options by default. Patient-specific predictions about adherence or side-effect risk lead to different drugs, different doses, and different monitoring plans.
When the model is well-calibrated, this can improve prescribing consistency and catch genuine contraindications. When it is not, physicians can end up following recommendations that do not fit the patient in front of them, often without knowing why the tool made that call.
What This Means for Pharma Teams
If AI tools are shaping which therapies make the shortlist, content that is not structured for how those systems process information may not reach the decision moment at all.
Clinical assets need clear patient selection criteria, organized safety profiles, comparative data, and switching guidance. Not because those elements are new, but because they now need to be legible to both the physician reading them and the AI layer they consulted before the visit.
The actual access problem for pharma and life science teams in Canada is no longer just whether a physician has heard of a therapy. It is whether it shows up, accurately and usefully, when an AI tool is narrowing what gets considered.
PharmaServ helps pharma and life science sales teams boost productivity with AI-powered workflows, real-time HCP insights, and compliant engagement.
Drive more calls, grow prescriptions, and make every connection count.
Contact
+12369785171
info@pharmaserv.co
4178 Dawson Street Burnaby British Columbia, Canada. V5C 0A1
Support
Policy
Copyright ©2026 PharmaServ